Jackson Kerbs
Projects ︎
The Inframent
Data Health
Age of fog
Design week
Bellwether
Obsidian
Client work ︎
Kubit.ai
Aurora Solar
Artbnk
Edify.ai
Fabric Eccomerce
Heliose
IQbar
Juicy Couture
Lore One
Starbucks
Tik Tok for Business
Ursa Major
WGU
Zillow
Explorations ︎︎︎
In Particulates ESS
The Oath
CanyonLands installation (SLC)
Prototyping_JAW
Privacy Suit
Surplus of Potential Situation
Biography ︎
Jackson is a Multi-disciplinary Designer, Concept Director, and Producer. His interests lie in the hidden truths that can be revealed through the investigation of human ecologies. Utilizing design thinking and grounded research, he informs his decisions in a derivative language of design.

Taking Care of Data
RESEARCH / 2018
From University of Utah
Download pdf ︎

Recently much of the public conversation in the news and media explores how ownership of personal data is defined; especially in the capital market. This is seen through national policy (General Data Protection Regulation, EU), multiple lawsuits (FB & HUD), and publicly broadcast Supreme Court hearings (Facebook 2018).
This project aims to apply questions of data ownership to healthcare, focusing on the patient’s relationship with their individual data. Do the policies and solutions to the free market apply personalized, data? How can the patient be empowered in their own health literacy without being exploited for the interests of the stakeholders at large? How might the lay person record and use their personal data to better understand health risks and diagnosis? And how might the primary care physician advocate for the careful use of data?
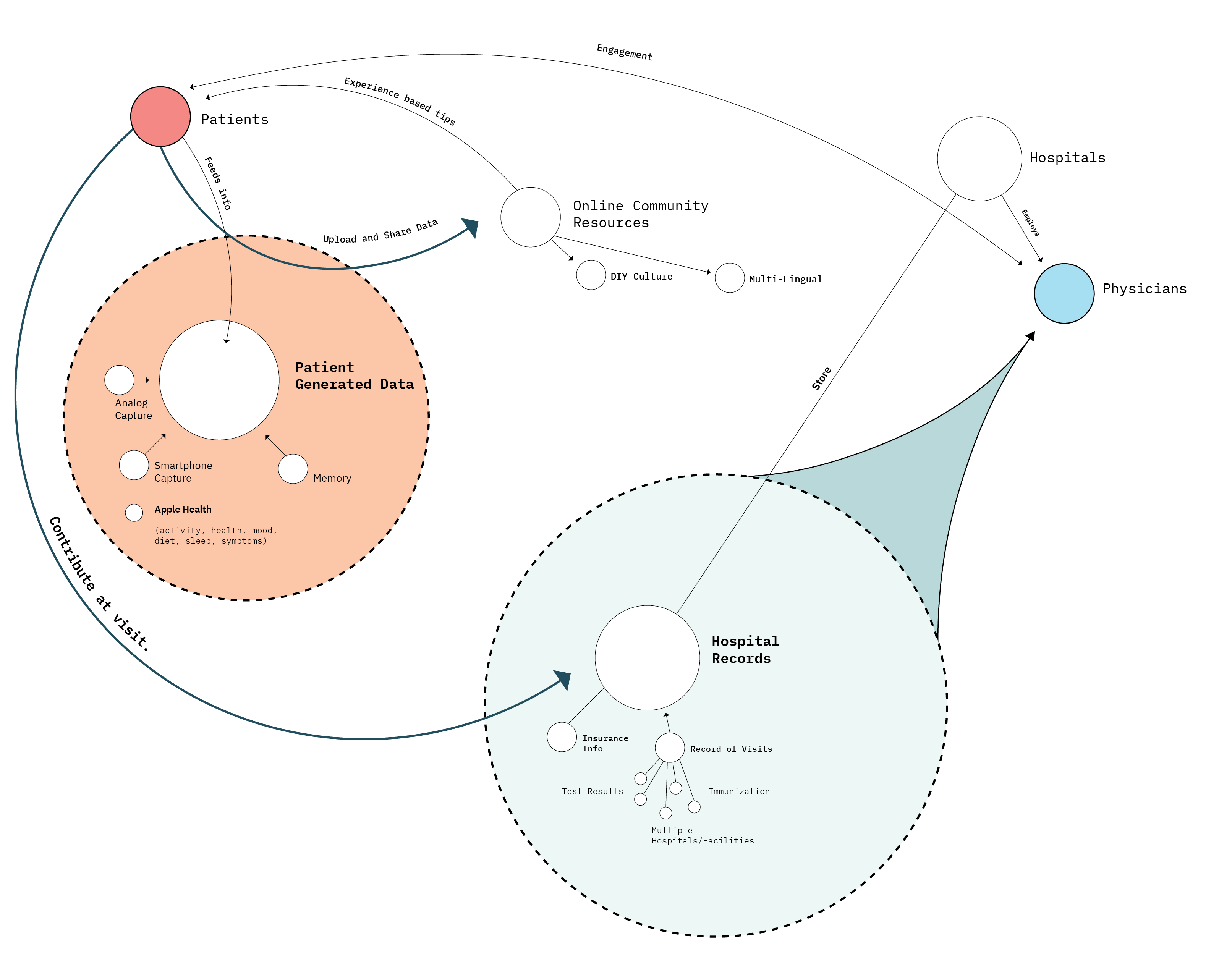
Knowledge Transfer Ecosystem
In order to understand the complexity in the Electronic Medical Record field, an ecosystem of entities within the field of “health knowledge transfer” was crafted including how each entity flows and relates to another. This map is made up of entities surrounding both the Patient and the Primary Care Physician and includes macro levels of data sharing and storage. The Diagram illustrates a distinct separation of Patient Generated Data and Hospital Records.

Patient Generated Data
In clinical practice patient generated data exists in forms of hospital records, insurance info and visit records. However the data from other capture methods are not currently being used in this area. How might the doctor facilitate the capture of usable patient data? Or is it the patients responsibility to collect and display their own data to their care provider.
In clinical practice patient generated data exists in forms of hospital records, insurance info and visit records. However the data from other capture methods are not currently being used in this area. How might the doctor facilitate the capture of usable patient data? Or is it the patients responsibility to collect and display their own data to their care provider.
Online Community Resources
Some patients use online communities, such as Twitter groups, to seek answers to questions their doctors aren’t addressing. The online presence offers support to its members because each member made up by someone with a direct connection to the topic issue.
Moderators of the communities validate the treatment recommendations. In 2006, researchers at the University of Texas analyzed the content from a breast cancer forum for medical accuracy. They found that 10 of the 4,600 postings contained false information. 7 of these posts were deleted leaving only 3 of the 4,600 posts to slip by uncorrected. (Suzanna Fox)
Some patients use online communities, such as Twitter groups, to seek answers to questions their doctors aren’t addressing. The online presence offers support to its members because each member made up by someone with a direct connection to the topic issue.
Moderators of the communities validate the treatment recommendations. In 2006, researchers at the University of Texas analyzed the content from a breast cancer forum for medical accuracy. They found that 10 of the 4,600 postings contained false information. 7 of these posts were deleted leaving only 3 of the 4,600 posts to slip by uncorrected. (Suzanna Fox)
One hour with a patient means two hours of entering data.
One intervention to the sharing of data is the area of Medical Scribes. A Scribe sits in physically or digitally to a patient visit and is solely responsible for the electronic notation of the patients chart. This frees up the physician to interact solely with the patient without bouncing between the patient and the electronic chart.
![]()
This works by using “Trigger Phrases.” When the doctor says something like “Your exam is normal except for...” this signals to the scribe that a note should be taken.
Now with advancing technology, with the patients permission, visits can be recorded with a multi-directional microphone. Then encrypted and transmitted through the Internet to a scribe overseas. The scribe makes notes to the health system and updates the patients file.

This works by using “Trigger Phrases.” When the doctor says something like “Your exam is normal except for...” this signals to the scribe that a note should be taken.
Now with advancing technology, with the patients permission, visits can be recorded with a multi-directional microphone. Then encrypted and transmitted through the Internet to a scribe overseas. The scribe makes notes to the health system and updates the patients file.

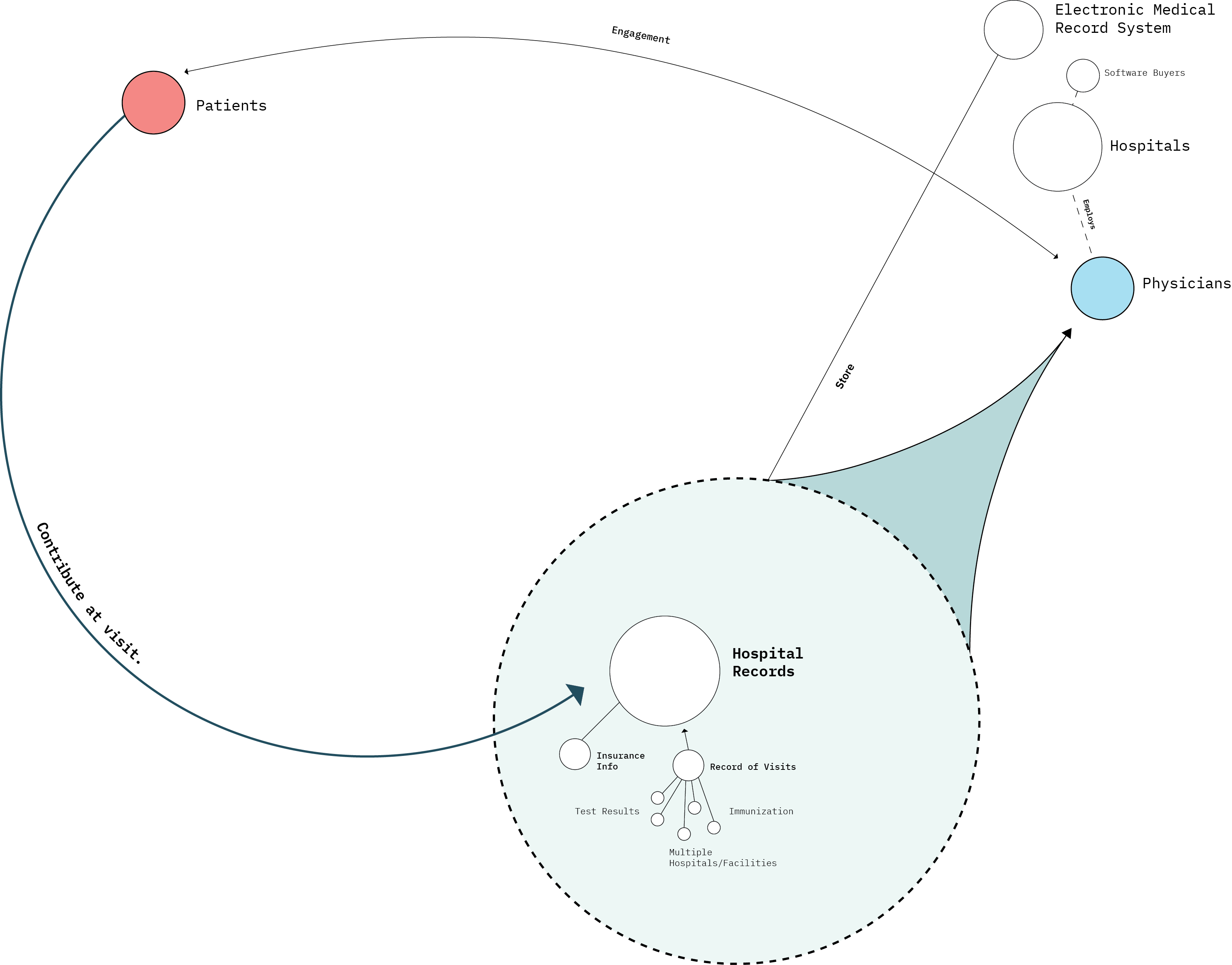
Data Access
The diagram above separates types of data that is only accessed using smart phone PGD and data types only accessible through the hospital system. Its important to note that much of the data on the right may be recorded in a smart phone, but the inherent procedural data is established in the facility of care. (Surgical, Immunization)
A Study in JAMA Network Open explores the difficultly of getting access to one’s Medical records. Dr. Harlan Krumholz, director of the Center for Outcomes Research and Evaluation at Yale New Haven Hospital in Connecticut, had trouble getting records for a family member so they decided to study the setbacks to record retrieval.
Krumholz examined 86 of the highest World Report ranked hospitals and explained to them that her grandmother was recently treated. She asked the hospitals a series of questions:
-
What was the procedure?
-
What was available?
-
How long would it take?
-
How much would it cost?
Of the 86 hospitals, 29 listed exact costs on a request form on their web page, 1 offered records free of charge, 18 said there would be a charge of some kind, and 36 didn’t specify.
Costs on forms ranged between $0.00 - $281.54
On the phone, 82 disclosed the cost. One hospital’s charged $541.50. This is quite a lot of money for records of a person’s property under HIPPA
Krumholz argues:
“But we don’t need to lobby legislators in Washington for this,” he said. “The law is clear. We need to get health systems in compliance with the law.”
Current Interventions
Digital Presence
87 % of 14-22 year olds have gone online for medical advice. The top three categories of interest being:
Fitness and exercise
Diet and Nutrition
Stress and Anxiety
The internet is becoming a place to seek diagnosis. These top three categories of information become apparent in Mobile Apps. Each using their own system to capture and use personal data.
This section will examine the current interventions of the digital space and personal health data. What is working? How? And What might work better?
Intervention Review
“Personal Health Narrative”
“Open Source Software”
“Symptom Checker”
“Personal Health Narrative”
“Open Source Software”
“Symptom Checker”
The Issue with Health Apps
“Symptom Checker” “Diagnosis” “Created by top Doctors” This is the messaging popular in the top grossing Health data apps. The issue here is that the usage of these apps can come with hidden terms of use that can compromise the user’s privacy.
How do lay people determine what commercial interests lie behind the apps’ development & how might their data be used?
“Symptom Checker” “Diagnosis” “Created by top Doctors” This is the messaging popular in the top grossing Health data apps. The issue here is that the usage of these apps can come with hidden terms of use that can compromise the user’s privacy.
How do lay people determine what commercial interests lie behind the apps’ development & how might their data be used?

This map shows the value transfer of stake holders at large. How does medical Tech advance from the digital products created in the consumer market? The map shows different types of value, monetary, information, advocation.
Oppurtunity Map
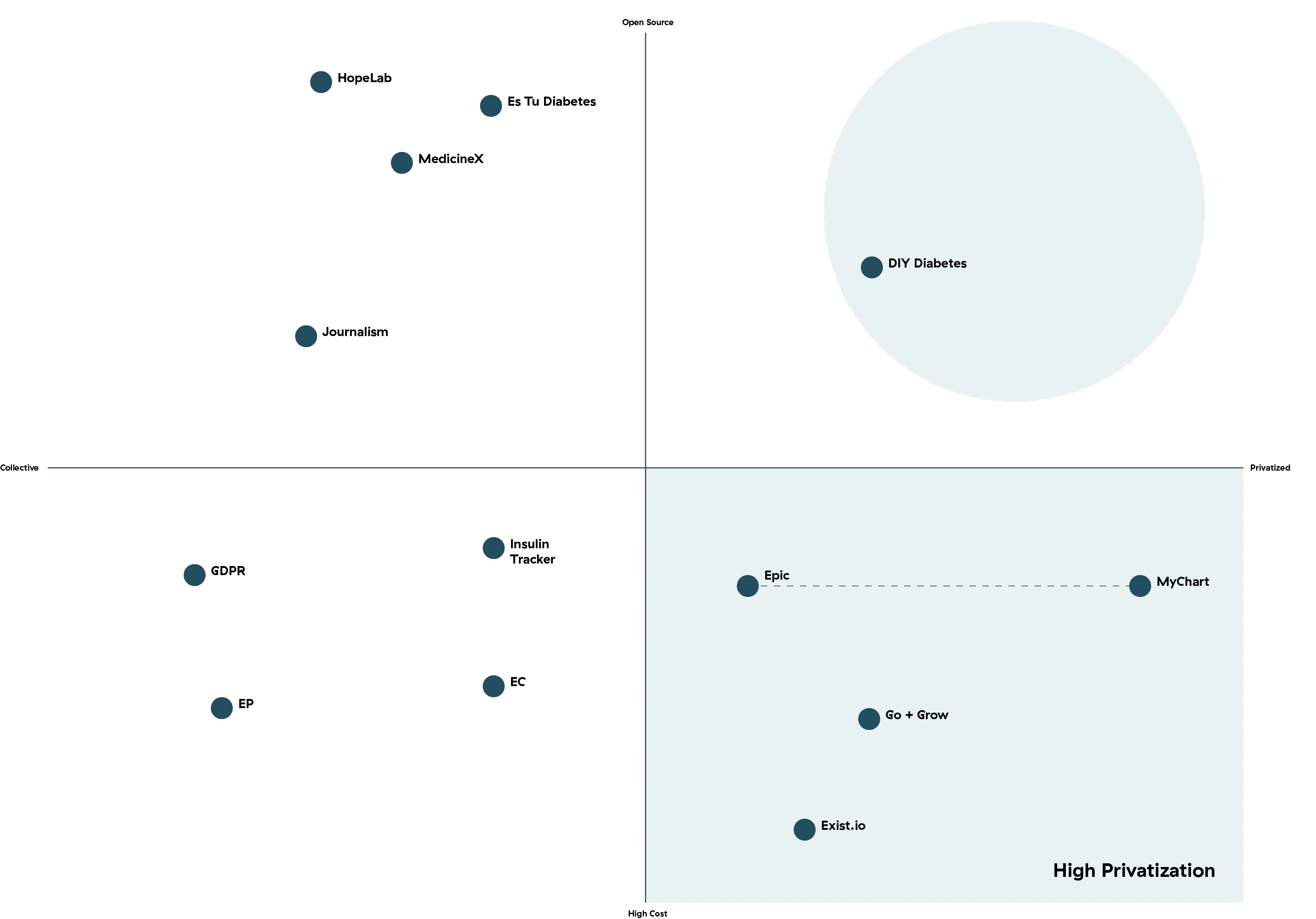
DIY Diabetes resides in an interesting place. The intervention utilizes open source programing and Private information to hack insulin readers to serve the purpose of the user. The users were upset with having to read insulin levels then administer the drug.
The solution was discovered not by doctors or designers, but by the users of the medication once they became more familiar with diabetic data and open source programming.
Strategy

Remote Access
Looking forward, it would be advantageous to see how data may be left in the hands of the individual, and how open-source technology may close gaps of health issues by eliminating restricted access. This section will illustrate some projections and models for design activity.
Digital Product comes with the advantage of remote access. An individual can use storage systems to archive important data and access instantly.
The diagram here shows one model of how the capture of data translates into a narrative with accessible literacy for the lay patient. By framing the insights as a Personal Health Narrative the individual is able to comprehend a personal story free of Medical Jargon.
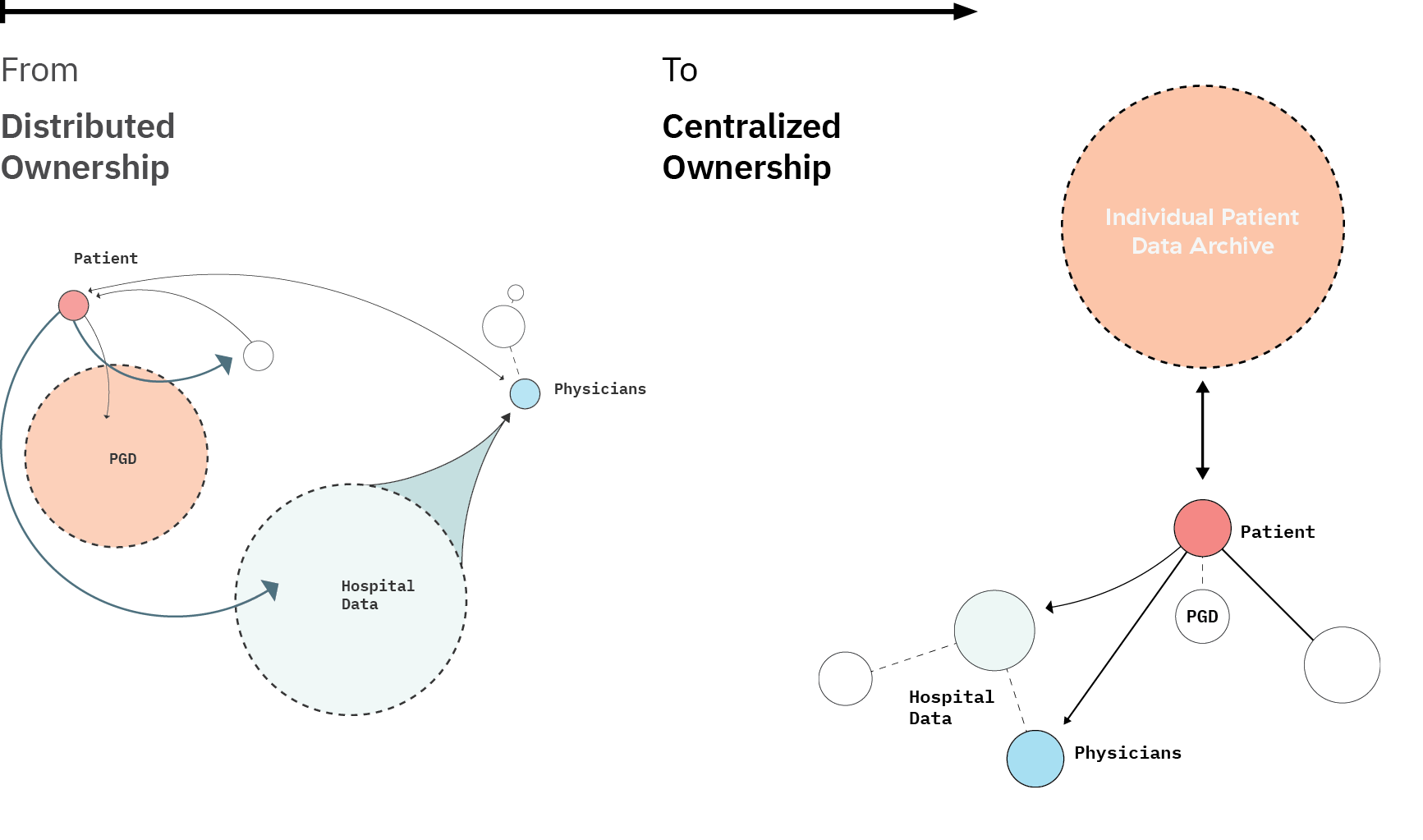
Patient Releases Data
How might we position data in the hands of the individual? This “future ecosystem” puts the data in the hands of the individual by creating an archive that the patients pulls information from and shares it conditionally to whom they decide. The Patient can share with Online community or hospital records as they please.
By reversing ownership from the EMR companies to the individual, the Patient becomes a more powerful stakeholder in the usage of their data.

Brief

| The patient’s personal data is at the core of this project and how the usage+access of more detailed data can aid diagnosis through primary care. Use PGD to enhance primary care diagnosis. The utilization of Data sharing to increase patient empowerment and engagement with their own health data capture and record. Advocate for the access and individual patient ownership of data. |
Download Pdf for Brief
Personal Reflection
Why don’t I have access to my medical records? This is the question that brought me to the area of health data ownership and privacy. I recently established new care with a hospital and was surprised by how there was no accessible record of my past immunizations. In order to get access to them I was told it would take 24 hours and I must sign a release of information agreement. This was all quite the process for something I felt was a quite simple ask.
During the visit I brought up my concerns with my physician and explained the opportunity for a design project. Soon I had 3 doctors in the room asking me how we could do it (make epic more legible.) While my blood was being drawn from arm.
Why don’t I have access to my medical records? This is the question that brought me to the area of health data ownership and privacy. I recently established new care with a hospital and was surprised by how there was no accessible record of my past immunizations. In order to get access to them I was told it would take 24 hours and I must sign a release of information agreement. This was all quite the process for something I felt was a quite simple ask.
During the visit I brought up my concerns with my physician and explained the opportunity for a design project. Soon I had 3 doctors in the room asking me how we could do it (make epic more legible.) While my blood was being drawn from arm.
Through my research I have become aware of a few things that have shaped my view of design research.
1. Field of view.
Global Health is a Monster Problem. It is important to frame a section of it and focus on it while allowing in outside perspective. I found this through the Data privacy question in this project. Privacy is different for everyone and is expressed through different ways but it wasn’t until I visited a physician myself that I formed and opinion on how my data should be handled. Sometimes it just takes a phone call or a meeting with someone close to you to become more involved in the issue.
2. The Treasure Hunt (Mine field)
Because the topic of discover was so big, I learned that an unwavering focus is a strong tool for tackling big issues. For every article you read, 10+ more questions can be asked to further your explorations. Those 10 questions lead you to 10 more readings, which lead to more questions. The cycle continues. It is with endless curiosity and gesture that I hope to find my solution.
Bibliography
(01+What+is+Design+for+Health_++(2).pdf, n.d.;
Contemporary Issues in Public Health in North Africa and the Middle East.pdf, n.d.;
COPub_SYR_August_2017_EN_19219.pdf, n.d.;
Botros, Perin, & Aseniero, n.d.;
Bryant, n.d.; Choe, Lee, Andersen, Wilcox, & Fitzpatrick, 2018;
El-Kak, 2013;
Feller et al., 2018;
LaRocca, Yost, Dobbins, Ciliska, & Butt, 2012;
Lund, 2018;
Luo & Kesselheim, 2015;
Lupton & Jutel, 2015; Rideout, n.d.; Stone, n.d.; Tseng, 2002;
Yeatts et al., 2012)
(Rideout, 2018.) Digital Health Practices, Social Media Use, and Mental Well-Being Among Teens and Young Adults in the U.S.
(2016. doi: 10.7326/M16-0961).
Apple Inc. “CareKit.” CareKit - Apple Developer, developer.apple.com/carekit/.
Carroll, Linda. “For U.S. Patients, Access to Medical Records Often Difficult and...” Reuters, Thomson Reuters, 9 Oct. 2018,
Gawande, Atul. “Why Doctors Hate Their Computers.” The New Yorker, The New Yorker, 24 Apr. 2019,
Twachtman, Gregory. “Study: One Hour with Patients Means Two Hours on EHR.” CHEST Physician, 3 Apr. 2019,